
Trial Design
The addition of IWILFIN maintenance therapy following standard of care upfront treatment1
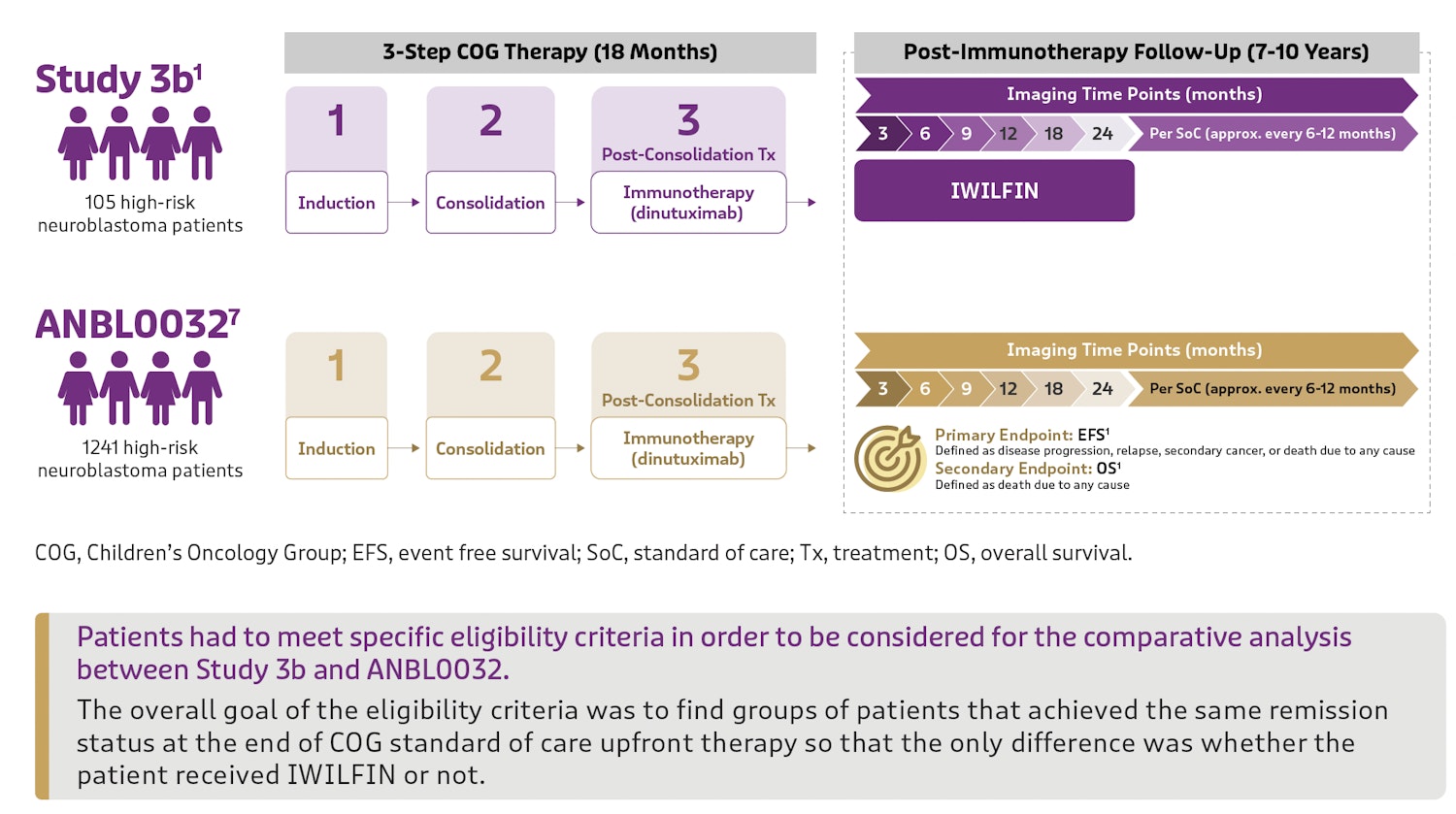
The efficacy of IWILFIN is based on an externally controlled trial comparison of outcomes between Study 3b (investigational arm) and Study ANBL0032 (clinical trial–derived external control arm).
- Study 3b (IWILFIN-treated patients): A multicenter, open-label, non-randomized trial. Pediatric patients with high-risk neuroblastoma who demonstrated at least a partial response to the standard of care upfront therapy, consistent with ANBL0032 treatment protocol, received IWILFIN orally twice daily for a maximum of 2 years
- Study ANBL0032 (external control): A multicenter, open-label, randomized trial of dinutuximab, granulocyte-macrophage colony-stimulating factor, interleukin-2, and cis-retinoic acid compared to cis-retinoic acid alone in pediatric patients with high-risk neuroblastoma
Comparing patient outcomes through propensity score matching2
Patients who met the criteria for the comparison and had complete data for specified clinical covariates were matched (1:3) using propensity scores; the matched efficacy populations for the primary analysis included 90 patients treated with IWILFIN and 270 control patients from ANBL0032.
Propensity Score Matching2
- Reduces biases when comparing data from different sources
- Balances baseline covariates between treated and control patients
- Optimizes similarity of compared groups
- Reduces confounding differences to better isolate treatment effect
Highly Similar Populations Used in Propensity Score Matching2
ASCT, autologous stem cell transplantation; CR, complete response; HRNB, high-risk neuroblastoma; INSS, International Neuroblastoma Staging System; PR, partial response; VGPR, very good partial response.
Efficacy
IWILFIN improved outcomes in primary matched comparison1,2
52% reduction in the risk of relapse with IWILFIN
Primary Endpoint: Event free survival (EFS)
EFS is defined as the period from the last day of immunotherapy until the first occurrence of relapse, progressive disease, secondary cancer, or death.

In supplementary analyses, the EFS HR ranged from 0.43 (95% CI: 0.23, 0.79) to 0.59 (95% CI: 0.28, 1.27). This equates to a reduced risk of relapse for patients taking IWILFIN that ranged from 57% to 41% respectively.
68% reduction in the risk of death with IWILFIN
Secondary Endpoint: Overall survival (OS)
OS is defined as the first day of administration of IWILFIN until death due to any cause.

In supplementary analyses, the OS HR ranged from 0.29 (95% CI: 0.11, 0.72) to 0.45 (95% CI: 0.21, 0.98). This equates to a reduced risk of death for patients taking IWILFIN that ranged from 71% to 55% respectively.
Safety
IWILFIN offers an established safety profile with manageable side effects1
Of 360 patients with high-risk neuroblastoma who received IWILFIN as maintenance therapy in clinical studies, IWILFIN was generally well tolerated
Adverse reaction rates (≥5%) in patients who received IWILFIN in a pooled safety population (n=360)
*13% of patients who received IWILFIN reported new or worsening hearing loss. Hearing loss was sometimes reversible with short-term does interruption and/or reduction. This percentage differs from what is included in the adverse reaction rates table as it takes into account additional pooled safety population analyses.
Most common (≥2%) grade 3 or 4 laboratory abnormalities (n=360)
ALT, alanine aminotransferase; AST, aspartate aminotransferase.
- Myelosuppression: Monitor blood counts before and during treatment with IWILFIN. Withhold, reduce dose, or permanently discontinue based on severity.
- Hepatotoxicity: Monitor liver function test before and during treatment with IWILFIN. Withhold, reduce dose, or permanently discontinue based on severity.
- Hearing Loss: Monitor hearing before and during treatment with IWILFIN. Withhold, reduce dose, or permanently discontinue based on severity.
- Embryo-Fetal Toxicity: IWILFIN can cause fetal harm. Advise females of reproductive potential of the potential risk to a fetus and to use effective contraception.
Based on the severity of adverse reactions to IWILFIN, reduce the patient’s dose or stop treatment until the reaction subsides or resolves to baseline1. Please see recommended dose reductions contained in the Prescribing Information.
References
1. IWILFIN. Prescribing information. USWM, LLC; 2024
2. Data on file. USWM, LLC.